Clinical outcomes after pulmonary vein isolation using an automated tagging module in patients with paroxysmal atrial fi
- PDF / 1,818,214 Bytes
- 8 Pages / 595.276 x 790.866 pts Page_size
- 98 Downloads / 292 Views
International Journal of Arrhythmia Open Access
RESEARCH
Clinical outcomes after pulmonary vein isolation using an automated tagging module in patients with paroxysmal atrial fibrillation Min Soo Cho, Jun Kim* , Ungjeong Do, Minsoo Kim, Gi‑Byoung Nam, Kee‑Joon Choi and You‑Ho Kim
Abstract Background: An automated tagging module (VISITAG™; Biosense Webster, Irvine, CA) allows objective demonstra‑ tion of energy delivery. However, the effect of VISITAG™ on clinical outcomes remains unclear. This study evaluated (1) clinical outcome after AF ablation using VISITAG™ and (2) the prevalence of gaps in the ablation line. Methods: This retrospective analysis included 157 consecutive patients (mean age, 56.7 years; 73.2% men) with par‑ oxysmal atrial fibrillation who underwent successful PVI between 2013 and 2016. Outcomes after the index procedure were compared between those using the VISITAG™ module (VISITAG group, n = 62) and those not using it (control group, n = 95). The primary outcome was recurrence of AF or atrial tachycardia after a blanking period of 3 months. Results: The VISITAG group showed significantly shorter overall procedure time (172.2 ± 37.6 min vs. 286.9 ± 66.7 min, P 30 s was documented on the electrocardiogram or Holter monitoring, either routine or symptom driven. The secondary outcome was the location and prevalence of VISITAG gap by each of
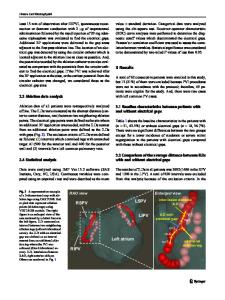
Fig. 2 Representative case of gap analysis. There were no gaps when using Criterion 1 (left), but gaps were noted when Criterion 2 was applied (right)
Cho et al. Int J Arrhythm
(2020) 21:13
Page 4 of 8
the three criteria. In addition, the rate of recurrent AF and AT was reassessed according to the presence or absence of VISITAG gap on the PVI line to assess the clinical impact of such gaps. Total procedure time, ablation time, fluoroscopic time, and procedure-related complications after PVI were also evaluated in the current study. All clinical outcomes were verified and adjudicated by an independent researcher. Statistical analysis
All statistical analyses were performed using R software (version 3.3.1; R Foundation for Statistical Computing, Vienna, Austria; www.r-project.org). All P values were two-sided, and P values 0.99 0.339
Previous medical history 0.823
Congestive heart failure
3 (1.9)
2 (2.1)
1 (1.6)
Vascular disease
4 (2.5)
3 (3.2)
1 (1.6)
Ischemic stroke/TIA
16 (10.2)
6 (6.3)
10 (16.1)
0.086
CHA2DS2-VASc score
1.2 ± 1.4
1.1 ± 1.4
1.4 ± 1.3
0.284
CHA2DS2-VASc score ≥ 2
54 (34.4)
28 (29.5)
26 (41.9)
0.151
Left ventricular ejection fraction, %
61.0 ± 6.3
61.0 ± 6.1
60.9 ± 6.7
0.905
Left atrial size, mm
39.6 ± 5.5
39.4 ± 4.9
39.9 ± 6.3
0.554
Left atrial volume, ml
112.5 ± 32.9
116.6 ± 31.8
108.0 ± 33.8
Amiodarone
14 (8.9)
8 (8.4)
6 (9.7)
Class 1C drug
120 (76.4)
68 (71.6)
52 (83.9)
0.114
Beta-blocker
47 (29.9)
22 (23.2)
25 (40.3)
0.034
Calcium channel blockers
47 (29.9)
32 (33.7)
15 (24.2)
0.275
Digoxin
10 (6.4)
2 (2.1)
8 (12.9)
0.018
BMI body mass index; TIA transient ischem
Data Loading...