Cytokine Responses in Severe Traumatic Brain Injury: Where There Is Smoke, Is There Fire?
- PDF / 1,048,903 Bytes
- 11 Pages / 595.276 x 790.866 pts Page_size
- 56 Downloads / 331 Views
REVIEW ARTICLE
Cytokine Responses in Severe Traumatic Brain Injury: Where There Is Smoke, Is There Fire? Colin Casault1,3* , Abdulaziz S. Al Sultan3, Mohammad Banoei1, Philippe Couillard1,3, Andreas Kramer1,3 and Brent W. Winston1,2 © 2018 Springer Science+Business Media, LLC, part of Springer Nature and Neurocritical Care Society
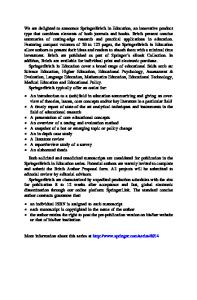
Abstract This scoping review will discuss the basic functions and prognostic significance of the commonly researched cytokines implicated in severe traumatic brain injury (sTBI), including tumour necrosis factor-α (TNF-α), interleukin-1β (IL-1β), IL-6, tissue inhibitor of matrix metalloproteinases-1 (TIMP-1), transforming growth factor-β (TGF-β), substance P, and soluble CD40 ligand (sCD40L). A scoping review was undertaken with an electronic search for articles from the Ovid MEDLINE, PUBMED and EMBASE databases from 1995 to 2017. Inclusion criteria were original research articles, and reviews including both animal models and human clinical studies of acute ( 220 ng/mL have a higher 30-day mortality [43]
Conflicting evidence, however, higher levels of IL-6 may have favorable outcomes [37] GG genotypes demonstrate higher levels of IL-6, which correlated with survival, whereas (-174C/G) polymorphism had the opposite [38].
Elevated CSF to serum ratio acutely is associated with an increased risk of developing PTE. Higher serum levels correlate with mortality [23, 31]
Higher levels correlate with mortality, multiorgan failure, increased risk of intracranial hypertension, and cerebral hypoperfusion [5, 13, 22]
Dual roles in secondary injury; acutely detrimental but beneficial in the subacute phase of injury in TBI [83]
TNF-α
Clinical data
Animal data
Biomarker
Table 1 Summary of the cytokines implicated in severe TBI
4
5
in the acute stage of sTBI. The combination correlated with an increased risk of hemorrhagic transformation (OR 4.6; CI 1.67–12.96; p = 0.004) [29]. The mechanism, while not entirely clear, is hypothesized to result from changes in the vascular wall integrity. Supportive research demonstrates homozygous IL-1R antagonist knockout (IL-1RA KO) mice experience premature death due to spontaneous hemorrhage. Histologic examination of the vascular wall in IL-1RA KO mice demonstrate uncontrolled vascular inflammation at sites of high vascular shear force as a potential contributing etiology [30]. IL-1β may also impact the development of post-traumatic epilepsy (PTE). Elevated CSF/serum IL-1β ratios during acute TBI are associated with an increased risk of developing PTE (HR 1.34, CI 1.08–1.67, p = 0.008) [31]. Additionally, IL-1β gene polymorphism may further impact epilepsy risk post-injury. TBI patients with heterozygous CT alleles of the rs1143634 genotype demonstrate a higher risk of epilepsy and shorter time to first seizure [mean = 854 days (759–949 days CI = 95%)] compared to those with CC or TT alleles [mean = 1011 days (959–1062 days p = 0.006)] [31]. Unsurprisingly, patients with elevated serum IL-1β levels at 6 and 12 h correlated with death after sTBI [23]
Data Loading...