Extra-articular Malunion of the Radius; Osteotomy of the Radius
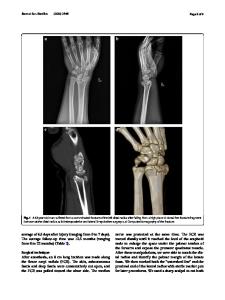
The most common radial deformity includes loss of palmar tilt, loss of inclination, loss of radial length, and a supination deformity of the distal fragment relative to the proximal diaphysis. In addition, the distal fragment may be displaced in a radial
- PDF / 517,118 Bytes
- 6 Pages / 504.57 x 720 pts Page_size
- 85 Downloads / 348 Views
37
Leiv M. Hove
Contents
37.1
37.1
Summary...................................................
37.2
Introduction ................................................ 300
37.3
Definition..................................................... 300
37.4
Anatomical Variables................................. 300
37.5
Preoperative Evaluation ............................ 300
37.6
Preoperative Planning ............................... 301
37.7
Timing ......................................................... 301
37.8
Technique for “Nascent” Malunion.......... 301
37.9
Technique for “Mature” Extra-articular Malunion ..................................................... 302
37.10
Outcome ...................................................... 302
37.11
Pearls and Pitfalls ...................................... 302
References ...............................................................
L.M. Hove, MD, PhD Department of Orthopaedic Surgery, Haukeland University Hospital, Bergen N-5021, Norway Department of Surgical Sciences, University of Bergen, Bergen, Norway e-mail: [email protected]
Summary
299
303
The most common radial deformity includes loss of palmar tilt, loss of inclination, loss of radial length, and a supination deformity of the distal fragment relative to the proximal diaphysis. In addition, the distal fragment may be displaced in a radial or ulnar translation and in a dorsal or palmar shift. Operative treatment is appropriate when the radiographic deformity correlates with a specific and anatomically correctable problem and if the deformity is associated with a substantial risk of dysfunction. The indication for operative correction is based on the combined appreciation of functional wrist impairment, the severity of pain, the grip strength, the degree of cosmetic deformity, and the radiographic findings. The planning of angular, rotational, and length corrections are based on preoperative radiographs of both wrists. Because radial shortening is a constant component of the deformity in both dorsal and volar malunion, an opening wedge osteotomy is recommended. This osteotomy should be transverse in the frontal plane and oblique (i.e. parallel to the joint surface) in the sagittal plane. In nascent malunion the intention is to “take down” the maturing callus and the “osteotomy” is performed at the site of the original fracture. After removing the callus, the fracture site is exposed, and the “osteotomy” may be performed with the knife or a small chisel into the fracture line.
L.M. Hove et al. (eds.), Distal Radius Fractures, DOI 10.1007/978-3-642-54604-4_37, © Springer-Verlag Berlin Heidelberg 2014
299
L.M. Hove
300
37.2
Introduction
Impaired function and pain after extra-articular malunion of distal radius fractures may be caused by derangements of the radiocarpal, ulnocarpal, and radioulnar joints. • Mal-alignment does not always result in dysfunction. In particular, the vast majority of older and physically low-demanding patients may function well with a wrist deformity. • In youn
Data Loading...