Giant circumflex artery aneurysm with arteriovenous fistula to the coronary sinus
- PDF / 3,278,846 Bytes
- 2 Pages / 595.276 x 790.866 pts Page_size
- 71 Downloads / 327 Views
IMAGES
Giant circumflex artery aneurysm with arteriovenous fistula to the coronary sinus Wildor Samir Cubas 1 & Héctor Bedoya-Copello 1 & Walter Llerena-Taco 1 & Lissette Aliaga-Sánchez 1 & José Ruiz-Peñafiel 1 Received: 4 August 2020 / Revised: 9 September 2020 / Accepted: 15 September 2020 # Indian Association of Cardiovascular-Thoracic Surgeons 2020
Abstract We present the extremely rare case of a circumflex artery aneurysm with an arteriovenous fistula to the coronary venous sinus in a 20-year-old male patient, requiring surgical management due to the clinical presentation of this unusual condition. Keywords Coronary artery fistula . Coronary artery aneurysm . Circumflex coronary artery . Coronary sinus
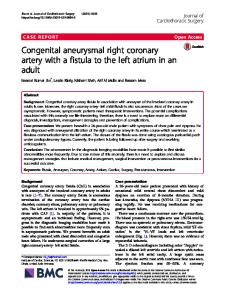
A 33-year-old man with no important medical history has presented intermittent anginal chest pain associated with mild dyspnea for 20 years. Chest radiography showed enlargement of the cardiac silhouette; echocardiogram, angiocoronography, and cardiac computed tomography showed dilatation of the right heart chambers and the left coronary trunk (22 mm) with the presence of a giant circumflex artery aneurysm (CAA) with a fistulous communication to the coronary sinus (Fig. 1, Video 1, Video 2). Surgical treatment was chosen, consisting of a median sternotomy with bicaval cardiopulmonary bypass and crossed aortic clamping. After identifying the CAA, it was ligated before its origin, in the proximal third of the left coronary trunk and at Electronic supplementary material The online version of this article (https://doi.org/10.1007/s12055-020-01062-4) contains supplementary material, which is available to authorized users. * Wildor Samir Cubas [email protected]; https://orcid.org/0000-0002-5380-7372 1
Department of Thoracic and Cardiovascular Surgery, Edgardo Rebagliati Martins National Hospital, Lima, Peru
the zone of the connection with the coronary sinus, and then, the aneurysmotomy was performed. The ostium of the left anterior descending artery (LAD) and the branches of the circumflex artery were identified within the aneurysm sac and immediately closed with continuous suture, excluding any connection site toward the aneurysm. Finally, coronary artery bypass graft (CABG) were performed, from the left internal mammary artery (LIMA) to the LAD and saphenous vein graft (SVG) to obtuse marginal artery (OMA). A CAA with arteriovenous fistula (AF) to the coronary sinus is extremely rare finding with an incidence of 0.02 to 0.2% [1, 2]. Unusual are the conditions for considering a CAA as “giant”; however, measures that quadruple its diameter (20–50 mm) have been proposed by the literature, despite the lack of consensus in this regard. This condition is frequently asymptomatic, but some patients may develop acute coronary syndrome, compression of surrounding structures, heart failure, and sudden death. Currently, the therapeutic strategy is not standardized, but may include conservative or surgical behavior [3].
Indian J Thorac Cardiovasc Surg Fig. 1 a Angiocoronography with evidence of dilation of the left ma
Data Loading...