Jejunogastric intussuception presenting as an epigastric mass: A rare case report
- PDF / 958,901 Bytes
- 3 Pages / 595.276 x 793.701 pts Page_size
- 37 Downloads / 297 Views
CASE REPORT
Jejunogastric Intussuception Presenting as an Epigastric Mass: A Rare Case Report Rashid Murtaza, Mritunjay Sarawagi, Shahid Murtaza, Saketan Bhagat
Abstract Jejunogastric intussusception is a potentially lethal complication of gastric surgery intussusceptions that can occur in any patient who has had a gastrojejunostomy. The diagnostic triad consists of high intestinal obstruction, left hypochondriac mass and hematemesis. On abdominal examination there may be left upper quadrant tenderness and guarding, and occasionally a mass may be felt. Often the mass is concealed by the rib cage and the guarding. Because the lesion is intraluminal, there is no peritoneal irritation and ileus is a late sign. This complication may occur at a variable period after original gastric operation. The treatment of acute variety of jejunogastric intussusception is prompt surgery. Delay in surgery beyond 48 hours is associated with an approximately 50% mortality. Key words: Jejunogastric intussuception; intussuception; gastrojejunostomy
Introduction
Case report
Jejunogastric intussusception is a potentially lethal complication of gastric surgery that can occur in any patient who has had a gastrojejunostomy. The diagnostic triad consists of high intestinal obstruction, left hypochondriac mass and hematemesis. Each of these signs may follow in progression. Paroxysms of nausea and vomiting of gastric contents occur initially. Gradually, the vomiting becomes “coffee grounds” and then bright red bleeding supervenes. Severe abdominal pain may be present. On abdominal examination there may be left upper quadrant tenderness and guarding, and occasionally a mass may be felt. Often the mass is concealed by the rib cage and the guarding. Because the lesion is intraluminal, there is no peritoneal irritation and ileus is a late sign.
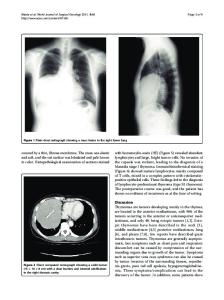
A 41-year-old female was admitted to the emergency ward of the Rajendra Institute of Medical Sciences, with complains of pain in the abdomen, vomiting and not passing stool or flatus since 3–4 days. Eight years earlier she had undergone surgery for peptic ulcer disease. Details of the operative procedure were not available by the patient. She had been asymptomatic until her recent admission to the emergency ward. A midline scar about 6 cm was present in upper abdomen. There was epigastric tenderness with a palpable mass. Laboratory investigations showed hemoglobin 9.0gm%, white cell count 8500/cmm with 76% polymorphs, 23% lymphocytes, and 1% eosinophils; blood sugar 90 mg%. Serum amylase and Urine analysis were normal. Plain X-ray of the abdomen showed multiple air fluid levels. USG suggested a colo-colic intussuception at splenic flexure. Initial treatment was resuscitative by intravenous fluids, blood transfusions and nasogastric suction. Laparotomy was planned. At laparotomy, gastrojejunostomy was found. A distended stomach filled with a soft mass was encountered. The presence of gastrojejunostomy (Figure 1, 2) was confirmed. The efferent jejunal loop was invaginating through the gastrojejunal stoma
Data Loading...