Laparoscopic extended right hemicolectomy with D3 lymph node dissection using a new articulating instrument
- PDF / 1,052,195 Bytes
- 3 Pages / 595.276 x 790.866 pts Page_size
- 25 Downloads / 326 Views
VIDEO FORUM
Laparoscopic extended right hemicolectomy with D3 lymph node dissection using a new articulating instrument H. Y. Jin1 · C. S. Lee1 · Y. S. Lee1 Received: 7 July 2020 / Accepted: 3 September 2020 © The Author(s) 2020
In this video, we show the use of an articulating laparoscopic instrument (ArtiSential®, LIVSMED, Inc., Republic of Korea) registered as a class I medical device with the Food and Drug Administration in 2019 and available since November 2019 in Korea (Fig. 1). Since the concept of complete mesocolic excision (CME) was introduced by Hoenberger et al. [1], CME with D3 lymph node dissection has been considered to improve oncologic outcomes. However, laparoscopic right hemicolectomy, including CME with D3 lymph node dissection, is technically challenging, particularly in ligation of the major vessels at their origin sites and lymphadenectomy along the superior mesenteric axis [2]. Obtaining the effective angle, traction, and countertraction is difficult using conventional straight-fixed laparoscopic instruments [3]. To overcome these limitations, a surgical robot system was introduced for colorectal surgery. Robot systems have the advantages of multi-joint instruments, ergonomics, and three-dimensional vision but are still expensive. As an alternative to robot systems, several laparoscopic articulating instruments have been introduced but are unfortunately not of practical use. In this video, we present laparoscopic extended right hemicolectomy using a new laparoscopic articulating instrument. The patient in the video is a 72-year-old woman with a body mass index of 23.3 kg/m2 at the time of surgery. She was diagnosed with a well-differentiated adenocarcinoma at the hepatic flexure of the colon. Initial computed tomography (CT) scan revealed clinical stage T3N1 and no evidence Electronic supplementary material The online version of this article (https://doi.org/10.1007/s10151-020-02345-z) contains supplementary material, which is available to authorized users. * Y. S. Lee [email protected] 1
Division of Colorectal Surgery, Department of Surgery, College of Medicine, Seoul St. Mary’s Hospital, The Catholic University of Korea, 222, Banpo‑daero, Seocho‑gu, Seoul 06591, Republic of Korea
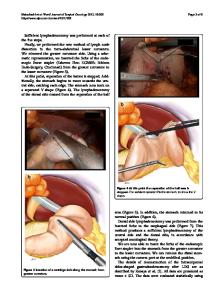
of distant metastasis. We performed laparoscopic extended right hemicolectomy with D3 lymph node dissection. The patient was placed in a modified lithotomy position with both arms along the body. A camera port was placed at the umbilicus, and three 5-mm ports were placed in the right lower quadrant, right upper quadrant, and left upper quadrant. An 8-mm port was placed in the left lower quadrant (Fig. 2). During the procedures, the surgeon used the ArtiSential® instrument through the left lower quadrant port and advanced surgical energy device (HARMONIC HD1000i, Ethicon, Cincinnati, OH, USA) through the left upper quadrant port (see video). Mobilization of the mesocolon was started from the ileocecal junction and dissected through the avascular plane between the mesocolon and the retroperitoneum usi
Data Loading...