Miller Fisher syndrome following meningococcal meningitis
- PDF / 669,731 Bytes
- 2 Pages / 595.276 x 790.866 pts Page_size
- 109 Downloads / 304 Views
LETTER TO THE EDITOR
Miller Fisher syndrome following meningococcal meningitis Lorna Stemberger Maric 1,2
&
Nina Krajcar 1 & Srdan Roglic 1 & Ana Tripalo Batos 3 & Goran Tesovic 1,4
Received: 26 January 2020 / Accepted: 23 July 2020 # Springer-Verlag GmbH Germany, part of Springer Nature 2020
Dear Editor: Neisseria meningitidis causes up to 40% of all cases of acute bacterial meningitis (ABM). Miller Fisher syndrome (MFS) is a rare clinical variant of cranial nerve GuillainBarré syndrome (GBS), characterized by a clinical trial of ataxia, areflexia, and ophthalmoplegia. There has been just one case report on Neisseria meningitidis-associated GBS so far [1]. To the best of our knowledge, this is the first case of MFS linked to meningococcal infection. An 11.5-year-old boy presented with 1 day history of fever, headache, and vomiting. Due to elevated inflammatory parameters (CRP 106 mg/L, WBC 35 × 109/L, with 80.6% of neutrophils) and positive meningeal signs, acute bacterial meningitis (ABM) was suspected. Cerebrospinal fluid (CSF) examination revealed neutrophilic pleocytosis (6827 cells per mm3), proteinorrachia (2.99 g/L), and mild hypoglycorrachia (CSF glucosis/blood glucosis 0.35). Nasopharyngeal swab revealed growth of Neisseria meningitidis group Y, and RT-PCR from CSF discovered the same microorganism. Brain CT scan performed at admission was normal. Treatment with ceftriaxone was continued and patient became afebrile within 48 h. Initially, the patient was somnolent with severe headache, but without localized neurologic signs and with normal deep tendon reflexes. His general condition improved over the next
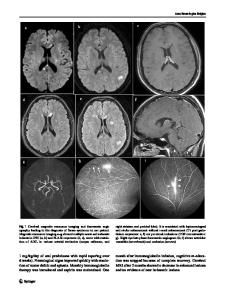
three days. Five days after admission, dyplopia and convergent strabismus occurred. Neurologic deficits in several days period progressed with bilateral (more on right eye) ptosis, inability of convergence on both eyes, left deviation of tongue, ataxia, and generalized arreflexia on lower extremities. Sinus bradycardia was noticed on ECG. Brain magnetic resonance imaging (MRI) showed intensive postcontrast enhancement of n.X bilaterally (dominantly left side), left n.IX, n.VIII bilaterally, n.III bilaterally (dominantly left side), and discrete imbibition of nuclei of n.XII bilaterally (dominantly left side), strongly suggestive for MFS (Fig. 1a–b). Antiganglioside antibodies (including IgG anti-GQ1b) were negative from serum taken at admission, as well as in serum after neurologic symptoms suggestive for MFS occurred. Serologic tests for Borrelia burgdorferi, tick-borne encephalitis (TBE) virus, Epstein-Barr virus (EBV), cytomegalovirus (CMV), Mycoplasma pneumoniae, and Bartonella henselae were all negative, as well as stool bacteriological cultures. The diagnosis of MFS was set and he was started on a 5-day course of therapeutic plasma exchange. Two days after initiation of the treatment, all his symptoms started to diminish and completely disappeared over the next 7 days. The patient was discharged after 14 days with completely normal clinical (including neurological) examination.
* Lorna Stemb
Data Loading...