Nerve Entrapments and Nerve Injuries in Distal Radius Fractures
There are four main nerves in the distal forearm and wrist: the median nerve, the ulnar nerve, the superficial radial nerve, and the posterior interosseous nerve. The most commonly affected nerve in distal radius fractures is the median nerve.
- PDF / 296,796 Bytes
- 5 Pages / 504.57 x 720 pts Page_size
- 26 Downloads / 354 Views
33
Adalsteinn Odinsson
Contents
33.1
33.1
Summary...................................................
271
33.2
Anatomy....................................................
272
33.3 33.3.1
Median Nerve ........................................... Acute Median Nerve Entrapment or Injury ..................................................... Late Median Nerve Entrapment ................. Superficial Radial Nerve Injury .................
272
Ulnar Nerve .............................................. Acute Ulnar Nerve Injury or Compression .......................................... Late Ulnar Compression Neuropathy in Guyon’s Canal .......................................
274
275
Posterior Interosseous Nerve Injury ......
275
References ...............................................................
275
33.3.2 33.3.3 33.4 33.4.1 33.4.2 33.5
A. Odinsson, MD Section of Hand Surgery, Department of Orthopaedic Surgery, St Olav’s University Hospital, Trondheim, Norway e-mail: [email protected]
272 273 273
274
Summary
There are four main nerves in the distal forearm and wrist: the median nerve, the ulnar nerve, the superficial radial nerve, and the posterior interosseous nerve. The most commonly affected nerve in distal radius fractures is the median nerve. The nerves may be damaged at the time of injury or in treatment of the fracture. This emphasizes the importance of a thorough examination and documentation of the neurovascular status prior to any treatment of the fracture and also after the treatment. This includes evaluation of sensibility and motor function. Nerve conduction studies can be of help in diagnosing and evaluating the nerve injury. In the acute phase, the nerve is affected by either a direct injury or an entrapment. Late nerve dysfunction is most often an entrapment of the nerve. In patients with a distal radius fracture and acute carpal tunnel syndrome, the fracture must be reduced and stabilized. Then the concomitant nerve compression syndrome will generally improve substantially over 24–48 h. If neurological symptoms increase or show no improvement after 1 or 2 days, carpal tunnel release is recommended with inspection of the nerve. It is important to remember that the compression or injury to the nerve may be in the carpal tunnel or 3 cm proximally, at the fracture site. An extended approach with adequately visualization and decompression at both sites is therefore recommended.
L.M. Hove et al. (eds.), Distal Radius Fractures, DOI 10.1007/978-3-642-54604-4_33, © Springer-Verlag Berlin Heidelberg 2014
271
A. Odinsson
272
33.2
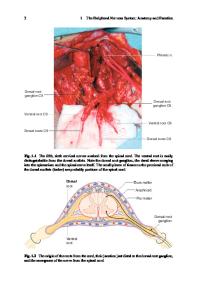
Anatomy
There are four main nerves in the distal arm and wrist: the median nerve, the ulnar nerve, the superficial radial nerve, and the posterior interosseous nerve (Figs. 33.1 and 33.2). The most commonly affected in distal radius fractures is the median nerve (Aro et al. 1988). Several authors have reported injury to the ulnar nerve in distal radius fractures, but the nerve is more at risk in distal forearm fractures when both radius and uln
Data Loading...