New insight of CMR in the diagnosis of left ventricular non-compaction: measurement of trabeculated left ventricular mas
- PDF / 635,435 Bytes
- 2 Pages / 610 x 792 pts Page_size
- 35 Downloads / 302 Views
BioMed Central
Open Access
Poster presentation
New insight of CMR in the diagnosis of left ventricular non-compaction: measurement of trabeculated left ventricular mass Alexis Jacquier*1, Franck Thuny1,2,3, Bertrand Jop1, Roch Giorgi1, Gilbert Habib1, Jean Michel Bartoli1 and Guy Moulin1 Address: 1CHU La Timone, Marseille, France, 2CHU la Timone, Marseille, France and 3CHU Timone, Marseille, France * Corresponding author
from 13th Annual SCMR Scientific Sessions Phoenix, AZ, USA. 21-24 January 2010 Published: 21 January 2010 Journal of Cardiovascular Magnetic Resonance 2010, 12(Suppl 1):P182
doi:10.1186/1532-429X-12-S1-P182
Abstracts of the 13th Annual SCMR Scientific Sessions - 2010
Meeting abstracts - A single PDF containing all abstracts in this Supplement is available here. http://www.biomedcentral.com/content/files/pdf/1532-429X-11-S1-infoThis abstract is available from: http://jcmr-online.com/content/12/S1/P182 © 2010 Jacquier et al; licensee BioMed Central Ltd.
Introduction Introduction: There is no universally accepted definition of left ventricular non compaction (LVNC) at present. Furthermore, investigators recently showed that there was a poor correlation between the 3 echocardiographic definitions of LVNC.
Purpose To describe a method for measuring trabeculated left ventricular (LV) mass using cardiac magnetic resonance imaging (CMR) and to assess its value in the diagnosis of LVNC.
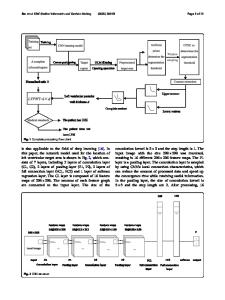
Methods Between January 2003 and 2008, we prospectively included 16 patients with LVNC. During the mean period we included 16 patients with dilated cardiomyopathy (DCM), 16 patients with hypertrophic cardiomyopathy (HCM), and 16 control subjects. All patients underwent a 1.5 T CMR with SSFP cine sequences, the following parameters were used: TR/TE = 40 ms/1.8 ms, slice thickness = 6 mm, no gap between slice, flip angle = 65°, matrix = 148 × 256, field of view = 350 × 350 mm, temporal resolution = 35 ms, retrospective gating for the Siemens scan; and TR/TE = 3.5/1.5 ms, slice thickness = 6 mm, no gap between slice, flip angle = 60°, matrix = 148 × 256, field of view = 350 × 350 mm, temporal resolution = 35 ms, retrospective gating for the Philips scan. LV volumes, LV ejection fraction and trabeculated LV mass were
measured (Figure 1). Figure 1: Illustration of the described method for measuring the global and trabeculated LV masses in patients with LVNC, DCM, HCM and controls. Row A shows the short axis end-diastolic cine images used for measurement without contouring. Row B shows inclusion of papillary muscles but exclusion of LV trabeculation for the measurements of the compacted LV mass. Row C shows inclusion of papillary muscles and trabeculation for the measurements of global LV mass.
Results The percentage of trabeculated LV mass was almost 3 times higher in the patients with LVNC (32 ± 10 %), compared to those with DCM (11 ± 4 %; P < 0.0001), HCM (12 ± 4 %, P < 0.0001), and controls (12 ± 5 %; P < 0.0001). A value of trabeculated LV mass above 20% of the global mass of the LV predicted the diagnos
Data Loading...