Paramedian Forehead Flap
- PDF / 1,970,217 Bytes
- 9 Pages / 439.37 x 666.142 pts Page_size
- 88 Downloads / 377 Views
16
Indications • Facial and nasal sof tissue defects Circulation • Axial by the supratrochlear artery Constituents • Fasciocutaneous: Skin and fascia overlying the forehead Contiguity • Local and regional Construction • Unipedicled Conditioning • Delay and subsequent two-stage reconstruction is possible. • Tissue expansion can be performed for large facial defects. Conformation • Fusiform or with the skin island oriented to the shape of the defect.
B.M. Erovic, P. Lercher, Manual of Head and Neck Reconstruction Using Regional and Free Flaps, DOI 10.1007/978-3-7091-1172-7_16, © Springer-Verlag Wien 2015
73
74
16 Paramedian Forehead Flap
A paramedian forehead flap harvest was first mentioned around 1500 BC in India. In Europe this flap has been described in the nineteenth century and the thirties of the twentieth century. The paramedian forehead flap has been popularized for nasal and face reconstruction.
Anatomy The forehead is determined superiorly by the hairline, inferiorly by the supraorbital ridge and eyebrows, medioinferiorly by the frontonasal groove, and laterally by the temporal bone. The skin overlying the forehead is not very mobile. The frontal muscle is an important part of the forehead.
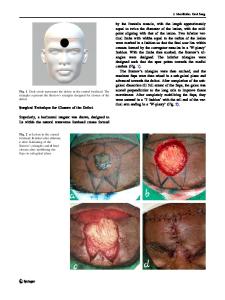
Blood Supply The paramedian flap is based on the supratrochlear artery, which is a terminal branch of the ophthalmic artery. The artery emerges from the orbital rim and is located 2 cm in the paramedian aspect from the midline of the forehead. The vessel is divided into a superficial and a deep branch. The superficial branch enters the galea 3.5 cm superior to the orbital rim into the frontal muscle. The deep branch courses with the subgaleal fascia 2–4 cm superior to the orbital rim (Fig. 16.1). 16.1
Preoperative Considerations
75
Innervation Supraorbital and supratrochlear nerves, which are branches of the trigeminal nerve, are responsible for sensory innervation of the forehead. The supraorbital nerve arises from the supraorbital foramen, while the supratrochlear nerves exit the orbit at the superior orbital rim. The frontal branch of the facial nerve ensures motor innervation of the forehead.
Indications The paramedian flap is a thin, axial fasciocutaneous flap. This flap is highly reliable, shows excellent tissue match, and is associated with low donor site morbidity. • Reconstruction of soft tissue defects after tumor excision: –– Facial and nasal defects. –– As a two stage procedure for large nasal/facial defects.
Advantages • Easy and quick harvesting of a very reliable and thin flap. • Excellent color and tissue match with the face.
Disadvantages • • • •
Patients’ poor acceptance of esthetics at the donor site. A second surgical procedure is needed in almost all cases. Scarring at the donor site. Hairy skin paddle at the distal tip of the flap.
Preoperative Considerations • Use a Doppler probe to identify the vascular pedicle. • Rule out previous surgery or trauma to the donor site.
76
16 Paramedian Forehead Flap
Surgical Steps 1. In this case a male patient with a recurrent basal cell c
Data Loading...