Clinical and ultrasonographical follow-up after standard removal of distal radius volar plates positioned distal to the
- PDF / 854,620 Bytes
- 5 Pages / 595.276 x 790.866 pts Page_size
- 21 Downloads / 312 Views
ORIGINAL ARTICLE
Clinical and ultrasonographical follow‑up after standard removal of distal radius volar plates positioned distal to the watershed line Chul Ki Goorens1,2 · Pieter‑Bastiaan De Keyzer1 · Jean François Goubau1,3 Received: 4 April 2020 / Accepted: 28 April 2020 © Springer-Verlag France SAS, part of Springer Nature 2020
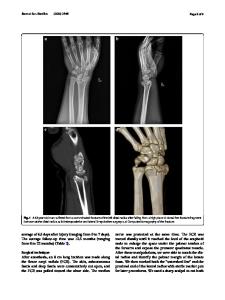
Abstract Marginal fracture types of the distal radius may require volar plate positioning distal to the watershed line. Subsequently, plate prominence with direct friction with the flexor tendons occurs which is associated with flexor tendon pathology. Standard plate removal can be proposed. This cohort study examined clinical outcome, patient satisfaction and ultrasonographical assessment of the relation of the flexor pollicis longus (FPL) and the volar rim after standard plate removal. Twenty patients with volar plate prominence after osteosynthesis for distal radius fractures were included. Plate removal was performed at least 4 months after initial surgery. The mean age was 60 years (range 39–84). The average delay from hardware removal to assessment was 2.9 years (range 1.0–5.0 years). Mean flexion, extension and radial deviation were significantly decreased (p 10°, radial shortening > 3 mm or translation > 3 mm. Three patients had already undergone subsequent surgery at the same wrist. Three patients had simultaneous dorsal plating, K-wire fixation or external fixation at initial surgery. One patient suffered from CRPS after initial osteosynthesis. We were not able to contact one patient. Two patients suffered from dementia, not able to complete the survey reliably. Lastly, two patients refused to participate, leaving 20 patients eligible for inclusion. At initial surgery, volar plating (volar rim and standard variable angle LCP Two-Column Distal Radius Plate 2.4, Depuy Synthes®, Oberdorf Switzerland) was performed by volar Henry approach. The pronator quadratus (PQ) was repaired in all patients by four resorbable interrupted double-mattress sutures (Vicryl 3.0, Ethicon®, Somerville, New Jersey). At plate removal, the same approach and dissection was used to access the osteosynthesis material. Remnant PQ repair was practically impossible due to
13
Inclusion criteria Age > 18 VLP removal > 4 months after osteosynthesis Absence flexor tendon rupture > 1 year follow-up Subtotal Exclusion criteria Soong Gr 0 plate prominence Malunion Subsequent surgery Dorsal plating/k-wire fixation Contralateral wrist surgery Major complications (CRPS, infection) Subtotal Loss to follow-up/dementia Refusal Subtotal Total
34 34 34 34 34 0 2 3 3 0 1 9 3 2 5 20
muscle adherence to the plate. No postoperative immobilization was used, and patients were instructed to initiate home exercise program, without physical therapy. Assessment was done at least one year after plate removal and consisted of range of motion (ROM) using a goniometer and grip strength using a hand dynamometer (Jamar Plus +; Sammons Preston®, Rolyon, Bolingbrook IL) and functional scoring with the short version of the Disabilities
Data Loading...