Overcoming the Barriers to Resident Engagement in Quality Improvement Initiatives in Psychiatry
- PDF / 240,707 Bytes
- 6 Pages / 595.276 x 790.866 pts Page_size
- 91 Downloads / 291 Views
COMMENTARY
Overcoming the Barriers to Resident Engagement in Quality Improvement Initiatives in Psychiatry Thomas O. Mitchell 1
&
Luming Li 1
Received: 4 August 2020 / Accepted: 26 October 2020 # Academic Psychiatry 2020
Despite it being 20 years since the Institute of Medicine reported poor quality and high variability in healthcare delivery [1], there are still significant opportunities for clinical quality improvement (QI). As frontline clinicians and future healthcare leaders tasked with driving these changes, resident physicians are an important cohort to equip with knowledge, skills, and experience in QI and patient safety (PS). The most recent iteration of the Accreditation Council for Graduate Medical Education (ACGME) competencies explicitly mandates that residents “receive training and experience in quality improvement processes” and “have the opportunity to participate in interprofessional quality improvement activities.” [2] A handful of psychiatry training programs have responded by redesigning or developing new QI curricula [3–6], though with limited descriptions of experiential project-based roles for residents. Active engagement in the experiential component of QI has been described as “a more powerful form of education than merely learning QI theory and processes.” [7] Similarly, the Kirkpatrick model for learning evaluation suggests that the application of knowledge into practice is an advanced way to display and solidify learning [8]. However, literature outside of psychiatry suggests that resident-led QI projects are frequently abandoned, unsuccessful, or unsustainable due to a multitude of barriers [9–11]. To our knowledge, only one project-based curriculum in psychiatry has reported sustained implementation of resident projects [6]. While the lack of project engagement can negatively impact residents’ educational development, it also represents a missed opportunity for their institutions, as trainees often have a unique and innovative perspective.
* Thomas O. Mitchell [email protected] 1
Yale University School of Medicine, New Haven, CT, USA
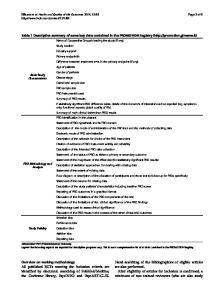
In this article, the authors review the barriers to resident engagement, leadership, and success with QI initiatives and propose potential solutions (see Table 1). Several barriers are unique to psychiatric training. The barriers described are broadly categorized as either structural or process-related, a distinction derived from Donabedian who described a framework for understanding the causal relationship between structures, processes, and outcomes in QI [12]. In addition, the authors provide an example of a resident-led QI initiative to illustrate the proposed solutions.
Structural Barriers to Engagement in Quality Improvement Barrier: Limited Quality Improvement Knowledge QI principles originated in manufacturing and business and have only recently been incorporated into medical training. A study surveyed residents regarding their QI involvement, finding a theme of “profound confusion about the QI process.” [13] They often misunderstand
Data Loading...