Risk of overconstraining femorotibial rotation after anatomical ACL reconstruction using bone patella tendon bone autogr
- PDF / 1,186,355 Bytes
- 8 Pages / 595.276 x 790.866 pts Page_size
- 41 Downloads / 296 Views
ARTHROSCOPY AND SPORTS MEDICINE
Risk of overconstraining femorotibial rotation after anatomical ACL reconstruction using bone patella tendon bone autograft M. Bernard1 · E. Pappas2 · A. Georgoulis3 · A. Haschemi1 · S. Scheffler4 · R. Becker5 Received: 29 March 2020 / Accepted: 30 September 2020 © Springer-Verlag GmbH Germany, part of Springer Nature 2020
Abstract Introduction Numerous studies have focused on the anteroposterior stability after anterior cruciate ligament (ACL) reconstruction, with less emphasis on rotational stability. It has been hypothesized that bone patella tendon bone (BTB) autograft for ACL reconstruction restores knee rotation closely to normal due to its comparable fiber orientation to the native ACL. Materials and methods Twenty patients with unilateral ACL rupture and an uninjured contralateral knee were included in this study. The ACL was reconstructed using the medial third of the patellar tendon. Tunnel placement was controlled by fluoroscopy. Implant-free press-fit graft fixation was used on both femoral and tibial side. Bone blocks were carefully placed to restore fiber orientation of both the anteromedial and posterolateral bundle, similar to the native ACL. Rotatory laxity of both knees was measured at 0° and 25° of flexion pre- and post-surgery, using an active opto-electronical motion-analysis system (LUKOTRONIC AS 100®). All measurements were performed under general anesthesia during surgery. Results Knee rotation was reduced significantly in both 0°and 25° of flexion following ACL reconstruction (p ICRS II. No additional cartilage procedure was performed. Meniscal injuries were found in 12 patients, which required partial resection (n = 9) or refixation (n = 3). Rotational stability was quantified with an optoelectronic motion-analysis system (LUKOtronic® AS 100, Lutz Kovacs-Electronics, Innsbruck, Austria). All measurements were carried out perioperatively under general anaesthesia by the same examiner prior and after ACL reconstruction. The study was reviewed by the Institutional Review Board of the Charitè, Berlin, Germany, and all patients gave written consent.
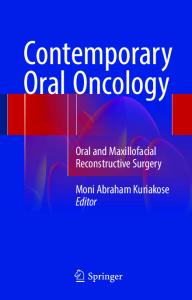
Surgical procedure A 10 mm-wide strip of the medial bone patellar tendon bone graft was harvested. Femoral tunnel placement was performed according to the quadrant methods by Bernard et al. [5] (Fig. 1). A K-wire was used to identify the correct aperture site confirmed by fluoroscopy. To create the tibial tunnel, a K-wire was placed in the center of the footprint of the native ACL and impingement was tested according to the technique described by Howell et al. before final tunnel preparation [15].
13
Fig. 1 Quadrant method (6): strictly lateral image, congruent overlay of both femoral condyles, quartering the sagittal diameter of the condyle and quartering the notch height. The center of the ACL insertion is located in the distal corner of the uppermost quadrant (blue arrow)
The graft was inserted through the anteromedial portal and the tibial bone block placed in the femoral tunnel flush with the latera
Data Loading...