A rare case of peritonitis in a young woman on peritoneal dialysis
- PDF / 468,524 Bytes
- 2 Pages / 595.276 x 790.866 pts Page_size
- 18 Downloads / 261 Views
LETTER TO THE EDITOR
A rare case of peritonitis in a young woman on peritoneal dialysis Yosuke Inaguma1 · Hiroshi Kaito1 · Ryojiro Tanaka1 Received: 17 May 2020 / Accepted: 18 June 2020 © Japanese Society of Nephrology 2020
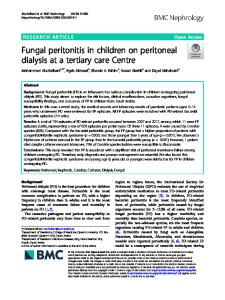
Keywords Acute abdominal pain · Bowel perforation · Peritoneal dialysis · Peritonitis To the editor, Patients on peritoneal dialysis (PD) with fever, abdominal pain, and cloudy peritoneal fluid are commonly suspected of PD-related peritonitis. Peritonitis due to bowel perforation in PD patients is comparatively rare and has few specific findings. A 19-year-old woman presented with fever and abdominal pain since the previous day. At birth, she was found to have deficiency of abdominal muscles, bilateral hypoplastic kidneys and anorectal malformations of persistent cloaca, which resulted in the diagnosis of prune belly syndrome (PBS). She was receiving automated PD since 14 years of age. Multiple intraperitoneal surgeries including sigmoid colostomy immediately after birth, transection of cloaca and permanent colostomy at 1 year of age, and abdominoplasty and colpoplasty at 4 years of age, had been performed before initiation of PD. She had experienced poorly controlled constipation. Vital signs on admission except for fever were normal. She was fully conscious, although she complained of severe pain and muscle guarding. There was no evidence of infection at the outlet and tunnel parts of the PD catheter. Laboratory tests revealed elevation of a white blood cell count and C-reactive protein level. Her peritoneal fluid was cloudy with leukocytosis (38,163/µL) and neutrophil predominance (80%). Feces and food residues could not be identified in it. Gram staining revealed a few of a single Gram-negative organism. The patient was diagnosed with PD-related peritonitis and immediately treated with intraperitoneal antibiotics. However, the abdominal pain progressively worsened. Computed tomography revealed sigmoid colon perforation and fecal mass (Fig. 1a). Emergency laparotomy * Hiroshi Kaito [email protected] 1
Department of Nephrology, Hyogo Prefectural Kobe Children’s Hospital, 1‑6‑7 Minatojima‑minamimachi, Chuo‑ku, Kobe, Hyogo 650‑0047, Japan
demonstrated advanced adhesion and dilation of the entire colon with massive feces. Gross examination of the resected specimen revealed a fecal mass in the part of the rectum nearest to the artificial anus (Fig. 1b). The final diagnosis was perforative peritonitis due to fecal impaction. Culture of the dialysis effluent revealed three bacteria types, including anaerobic bacteria. Peritonitis due to bowel perforation is a fatal condition with a high mortality rate [1]. Although it requires immediate surgical intervention, perforative peritonitis in PD patients is often difficult to diagnose early. PD patients with bowel perforation sometimes exhibit feculent dialysate or watery diarrhea containing dialysate [2]. Multiple or anaerobic bacteria in peritoneal fluid could be a key feature of bowel perforation [3], but the results can be confirm
Data Loading...