Chylous Ascites
- PDF / 325,501 Bytes
- 2 Pages / 595.276 x 790.866 pts Page_size
- 29 Downloads / 296 Views
Department of Medicine, University of California, San Francisco, San Francisco, CA, USA; 2School of Medicine, University of California, San Francisco, San Francisco, CA, USA; 3Department of Medicine, University of California, San Francisco, CA, USA; 4San Francisco VA Medical Center, San Francisco, CA, USA.
J Gen Intern Med DOI: 10.1007/s11606-019-05532-3 © Society of General Internal Medicine 2019
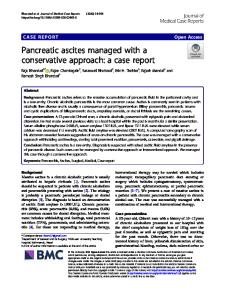
69-year-old man with HCV cirrhosis and newly diagA nosed diffuse large B cell lymphoma was admitted for chemotherapy. He had a distended abdomen and an abdominal ultrasound revealed ascites. Paracentesis yielded 2 l of pink, milky-appearing ascitic fluid that separated into two layers, with a white layer on top (Fig. 1). Ascitic fluid triglycerides were 330 mg/dl. The diagnosis of chylous ascites should be suspected when ascitic fluid appears milky and is established when the ascitic fluid triglyceride level is > 200 mg/dl.1, 2 In developing countries, infection is the most common cause, including tuberculosis and filariasis.1 In developed countries, the most common causes are abdominal malignancy and cirrhosis with lymphoma being responsible for approximately 8% of cases in adults.1, 3 The mechanism of action of chylous ascites due to lymphoma is obstruction of lymphatic drainage secondary to lymphadenopathy, causing exudation of chyle.4 This patient’s significant retroperitoneal lymphadenopathy visualized on
Received July 17, 2019 Revised October 4, 2019 Accepted October 28, 2019
PET/CT (Fig. 2) likely caused obstruction of the cisterna chyli that receives lymphatic drainage in the abdomen. The mainstay of management of chylous ascites is treatment of the underlying condition. This patient received chemotherapy with R-CHOP for treatment of his lymphoma. A low-fat diet with medium-chain triglyceride supplementation is also generally recommended.5, 6
Figure 1 Milky-appearing ascitic fluid immendiately following paracentesis (left), and several hours later separating into two distinct layers (right).
Corresponding Author: Elizabeth Adler, MD; Department of Medicine University of California, San Francisco, San Francisco, CA, USA (e-mail: [email protected]).
Compliance with Ethical Standards: Conflict of Interest: The authors declare that they do not have a conflict of interest.
REFERENCES 1. 2.
3.
4. 5.
6.
Figure 2 PET/CT coronal section demonstrating enlarged retroperitoneal lymph nodes (fused arrows).
Cárdenas A, Chopra S. Chylous Ascites. Am J Gastroenterol. 2002;97(8):1896-900. Bhardwaj R, Vaziri H, Gautam A, Ballesteros E, Karimeddini D, Wu GY. Chylous Ascites: A Review of Pathogenesis, Diagnosis and Treatment. J Clin Transl Hepatol 2018;6(1):105-113. Steinemann DC, Dindo D, Clavien P-A, Nocito A. Atraumatic chylous ascites: systematic review on symptoms and causes. J Am Coll Surg 2011;212(5):899-905-4. Aalami OO, Allen DB, Organ CHJ. Chylous ascites: a collective review. Surgery. 2000;128(5):761-778. Hashim SA, Roholt HB, Babayan VK, Van Itallie TB. Treatment of Chyluria and Chylothorax with Mediu
Data Loading...