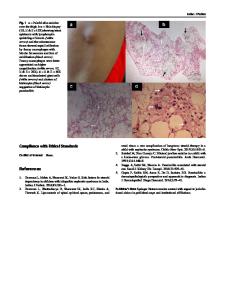
Chylous Ascites in Nephrotic Syndrome
- PDF / 259,844 Bytes
- 1 Pages / 612 x 792 pts (letter) Page_size
- 50 Downloads / 295 Views
Chylous Ascites in Nephrotic Syndrome
Chylous accumulation in peritoneal cavity may be caused by intestinal lymphangiectasia which may be congenital or associated with trauma, lymphoma, intestinal malignancy, pancreatitis, liver cirrhosis liver and right-sided heart failure [1]. Chylous ascites is not commonly a feature of idiopathic nephrotic syndrome in children.
A
scites is a common feature in children with nephrotic syndrome, and if not treated early, it may gradually increase. The fluid is a transudate with a very low protein content and few cells. Occurrence of chylous ascitic fluid has been occasionally reported in adult patients with nephrotic syndrome, usually being caused by obstruction to lymphatics [1]. We report the case of a child with steroid resistant nephrotic syndrome (SRNS) who developed massive ascites. Paracentesis revealed the chylous nature of the fluid. Such a feature is rare and not well explained. A 6-year-old child with SRNS was referred to us for with massive ascites, respiratory distress and oliguria. He was diagnosed 1 year back with SRNS, following no response to the standard treatment with prednisolone (2 mg/kg daily for 6 weeks followed by 1.5 mg/kg on alternate days for 6 weeks). A renal biopsy was advised but declined by the parents seeking alternative treatment. The child developed abdominal distension about 8 months back, which had recently increased significantly to cause difficulty in breathing and decreased urine output. There was no associated history of jaundice or upper gastrointestinal bleeding or any other systemic illness.
Examination showed a severely malnourished child with massive ascites respiratory distress, facial and pedal edema, marked pallor and cold peripheries. Vitals revealed tachycardia, tachypnea and a blood pressure of 80/40 mmHg. On laboratory evaluation the hemoglobin was 6.2 g/dL, serum albumin 1.4 g/dL, globulin 1.4 gm/dL, urea 101mg/dL and creatinine 1.7 mg/dL. The levels of serum electrolytes, bilirubin and liver enzymes were within normal range. Fasting lipid profile including serum cholesterol (138 mg/dL) was normal. Urine showed 4+ protein and no red cells on microscopy. Fluid resuscitation was done with 0.9% saline following which peripheral perfusion improved but oliguria persisted (urine output 100 ml in first 24 hour). He was given 20% albumin infusion and diuretics. Abdominal paracentesis was done to relieve respiratory distress. Paracentesis revealed milky white fluid, which on analysis showed protein content of 1.2 gm/dL and triglycerides of 145 mg/dL. Microscopy showed 110 cells/mm3, mostly lymphocytes and predominant chylomicrons. The culture of the fluid was sterile.
A few isolated cases of chylous ascites have been described in adults with nephrotic syndrome with membranous nephropathy [2], focal segmental glomerulosclerosis [3] and renal vein thrombosis [4]. Recently chylous ascites was reported as a presenting feature in a child with systemic lupus [5]. In our patient various secondary causes of nephritic syndrome were excluded.
Data Loading...