Discontinuation of rLH two days before hCG may increase the number of oocytes retrieved in IVF
- PDF / 175,961 Bytes
- 3 Pages / 595.276 x 793.701 pts Page_size
- 93 Downloads / 315 Views
METHODOLOGY
Open Access
Discontinuation of rLH two days before hCG may increase the number of oocytes retrieved in IVF Jessica B Spencer1*, Aimee S Browne1, Susannah D Copland2, Donna R Session1
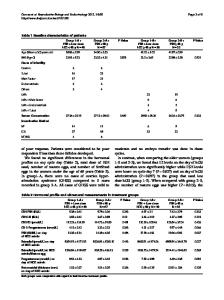
Abstract Background: Administration of recombinant luteinizing hormone (rLH) in controlled ovarian hyperstimulation may benefit a subpopulation of patients. However, late follicular phase administration of high doses of rLH may also reduce the size of the follicular cohort and promote monofollicular development. Methods: To determine if rLH in late follicular development had a negative impact on follicular growth and oocyte yield, IVF patients in our practice who received rFSH and rLH for the entire stimulation were retrospectively compared with those that had the rLH discontinued at least two days prior to hCG trigger. Results: The two groups had similar baseline characteristics before stimulation with respect to age, FSH level and antral follicle count. However, the group which had the rLH discontinued at least two days prior to their hCG shot, had a significantly higher number of oocytes retrieved, including a higher number of MII oocytes and number of 2PN embryos. Conclusions: When using rLH for controlled ovarian hyperstimulation, administering it from the start of stimulation and stopping it in the late follicular phase, at least two days prior to hCG trigger, may increase oocyte and embryo yield.
Background The precise benefit and use of recombinant luteinizing hormone (rLH) is still debated. It is unclear which subpopulation benefits the most (e.g. poor responders, extreme pituitary suppression, patients with anovulation). Routine administration of rLH in antagonist cycles may increase the peak serum E2 level but did not increase the number of oocytes retrieved or increase IVF pregnancy rates in one large randomized controlled trial [1]. A recent case-control study however did show a significant increase in implantation rates when rLH was used with antagonist cycles [2]. Adding rLH after day 6 of stimulation in a favorable prognosis population does not seem to improve stimulation or pregnancy rates either [3,4]. However, when an undesirable response occurs after initial stimulation with FSH alone, adding rLH rather than increasing the FSH dose may increase the number of oocytes retrieved [5] and possibly the pregnancy rate per transfer [6]. The optimal * Correspondence: [email protected] 1 Division of Reproductive Endocrinology & Infertility, Department of Gynecology & Obstetrics, Emory University School of Medicine, Atlanta, GA, USA
dose and timing of rLH in controlled ovarian hyperstimulation is also unclear. One efficacy study showed an increased pregnancy rate with 75 IU vs. 37.5 IU daily (31% vs. 21% respectively) [7]. While the addition of rLH may increase response in COH, very high doses of rLH (660 IU/day) in anovulatory women, who are at particular risk of ovarian hyperstimulation, may promote the growth of a single dominant follicle [8], thereby reducing her risk for ovarian hyperstimulation syndrome.
Data Loading...