Clinical evaluation of inline motion correction for cardiac perfusion MRI
- PDF / 252,423 Bytes
- 2 Pages / 595.276 x 793.701 pts Page_size
- 71 Downloads / 318 Views
POSTER PRESENTATION
Open Access
Clinical evaluation of inline motion correction for cardiac perfusion MRI Aya Kino1*, Christopher Glielmi2, Mauricio S Galizia1, Andrada R Popescu1, Hui Xue3, Jens Guehring Guehring3, Peter Weale2, Sven Zuehlsdorff2, James C Carr1 From 2011 SCMR/Euro CMR Joint Scientific Sessions Nice, France. 3-6 February 2011 Objective The purpose of this study is to evaluate the impact of non-rigid registration of cardiac perfusion images on image quality and diagnostic accuracy. Background Cardiac MR is often utilized to assess myocardial perfusion [1].Typically, T1 weighted images of the first pass of contrast agent are qualitatively assessed to identify hypo-enhanced regions of the myocardium. Although fully integrated approaches are available to register individual images to eliminate motion the impact on diagnostic accuracy has not been validated in patients [2]. Materials and methods Cardiac stress and rest first pass perfusion images (SR prepared TFL, 160×131 matrix, 2.8x2.3x10 mm spatial resolution, TI =100 ms, TE/TR =1.05/2.1 ms, TGRAPPA factor 2) were acquired in eight patients with suspected ischemic heart disease on a clinical 1.5T scanner (MAGNETOM Avanto, Siemens Healthcare). Three short axis slices were acquired during infusion of 0.075 mMol/kg
of Gadolinium (Magnevist, Bayer HealthCare Pharmaceuticals, USA) at rate of 4 ml/sec. Using a conventional clinical protocol, patients were instructed to breath-hold during the beginning of the scan and resume shallow breathing after 30 hearts beats. Stress scans consisted of adenosine (Adenoscan, Astellas Pharma, USA) infusion (0.14 mg/kg/min; rate: 0.2 cc/sec; 4 min). In addition to motion correction, inline processing also consisted of temporal filtering and surface coil correction [2].Conventional and motion-corrected images were assessed by 2 radiologists using the AHA 16-segment model and scored using a four point Likert scale (1-poor/nondiagnostic; to 4-excellent without artifacts) for each slice. Signal intensity curves in each segment from both methods were normalized by baseline signal intensity of the left ventricle.
Results Eight patients were successfully scanned; perfusion defects were detected in 2 patients. The mean image quality score for motion corrected images (3.76 ± 0.34) was superior to conventional images (2.59 ± 0.46)
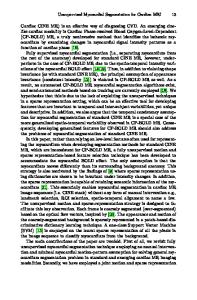
Figure 1 A) Time course for segment affected by surface coil correction (segment 5 AHA). B) Time course for segment less affected by this correction (segment AHA). 1 Northwestern University, Chicago, IL, USA Full list of author information is available at the end of the article
© 2011 Kino et al; licensee BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Kino et al. Journal of Cardiovascular Magnetic Resonance 2011, 13(Suppl 1):P54 http://jcmr-online.com/cont
Data Loading...