Extracapsular Spread in Melanoma Lymphadenopathy: Prognostic Implications, Classification, and Management
- PDF / 676,888 Bytes
- 12 Pages / 595.276 x 790.866 pts Page_size
- 62 Downloads / 295 Views
ORIGINAL ARTICLE – MELANOMA
Extracapsular Spread in Melanoma Lymphadenopathy: Prognostic Implications, Classification, and Management Michelle Lo, MRCS1, Alyss Robinson, MRes2, Ryckie Wade, MRCS2,3, Howard Peach, FRCS(Plast)3, Donald Dewar, FRCS(Plast)3, Martin Heaton, FRCS(Plast)1, and Marc Moncrieff, FRCS(Plast)1,4 1
Department of Plastic and Reconstructive Surgery, Norfolk and Norwich University Hospital, Norwich, UK; 2Faculty of Medicine and Health, University of Leeds, Leeds, UK; 3Department of Plastic and Reconstructive Surgery, Leeds Teaching Hospitals NHS Trust, Leeds, UK; 4Norwich Medical School, University of East Anglia, Norwich, UK
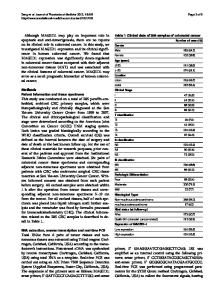
ABSTRACT Background. Extracapsular spread (ECS) is recognized to be a high-risk factor in melanoma patients with macrometastatic (N?) nodal disease; however, ECS risk in sentinel lymph node (SLN) biopsy, micrometastatic stage III disease is ambiguous. Objective. The aim of this study was to examine ECS incidence and its prognostic significance. Methods. A two-center, retrospective analysis of all patients with micro/macrometastatic lymphadenopathy undergoing nodal surgery from 2008 to 2014 was performed. Patient demographics, tumor characteristics, nodal ECS status, and patient outcomes were collected. Results. Overall, 515 patients with nodal disease were identified (males/females = 277/238); median age was 63 years (range 17–94). There was an increased frequency of ECS disease in N? disease compared with SLN? disease (52.4% vs. 16.2%; p \ 0.0001). The absolute diseasespecific survival (DSS) difference for SLN? patients was approximately 30% at 10 years (66.2% vs. 37.2%; p \ 0.0001), and the prognosis of SLN?/ECS? patients was identical to N?/ECS- patients. Multivariate analysis demonstrated that ECS status was an independent prognostic indicator for DSS (hazard ratio 2.47, 95% confidence interval 1.87–3.26; p \ 0.0001) in patients with SLN? disease. There were significant differences in nodal
Ó Society of Surgical Oncology 2020 First Received: 9 November 2019 Accepted: 15 August 2020 M. Lo, MRCS e-mail: [email protected]
burden according to ECS status between the SLN? and N? subgroups suggestive of differing biology in ECS? tumors. Conclusion. We found that ECS is a significant DSS, progression-free survival, and overall survival indicator in SLN? and N? disease. We demonstrated that ECS upstages stage III disease, similar to ulceration in primary melanoma (stage I/II disease). A simplified staging system substituting ECS for N stage accurately stages patients according to prognosis.
The American Joint Committee on Cancer (AJCC) 8th edition staging system1 has produced some significant changes in the classification of melanoma, in particular the stage III group. For the first time, stage III not only incorporates data from the ‘N’ stage but also qualifying ‘T’ data from the primary, such as Breslow thickness and ulceration status. This takes into account the fact that the risk of distant spread and subsequent death from melanoma of the stage III group is dependent o
Data Loading...