Pharmacotherapy and the Frailty Syndrome
As outlined in chapter “Heterogeneity and Vulnerability of Older Patients,” the frailty syndrome is a major feature to categorize elderly persons according to their vulnerability, prognosis, and risk-benefit ratio under the particular aspect of diagnostic
- PDF / 200,378 Bytes
- 7 Pages / 504.567 x 720 pts Page_size
- 52 Downloads / 339 Views
Introduction As outlined in chapter “Heterogeneity and Vulnerability of Older Patients,” the frailty syndrome is a major feature to categorize elderly persons according to their vulnerability, prognosis, and risk-benefit ratio under the particular aspect of diagnostic and therapeutic interventions. Therefore, it also serves as one of the most important patient characteristics to guide differential pharmacotherapy in the elderly. The frailty syndrome describes a frequent phenotype at advanced age and refers to pathophysiologic cascades attributable to the aging process. Frailty identifies elderly persons with both reduced resources and altered body composition, factors most significant for changes in pharmacokinetics and pharmacodynamics.
Definition of the Frailty Syndrome and Underlying Mechanisms A major characteristics of the apparent heterogeneity of the elderly is the wide range of physical fitness levels. Elderly with apparently impaired fitness and evident vulnerability are denominated as frail. In the field of geriatrics, the frailty
H. Burkhardt (*) IVth Department of Medicine, Geriatrics, University Medical Centre Mannheim, Theodor-Kutzer-Ufer 1-3, Mannheim 68167, Germany e-mail: [email protected]
syndrome was defined to identify elderly at risk for advanced aging processes and increased mortality and morbidity. The frailty syndrome describes – Increased vulnerability to different stressors – Decreased functionality, especially regarding locomotion – Impaired compensatory resources. Although this phenotype is seemingly well known and described from a clinical point of view, a precise identification and classification is difficult due to missing or ill-defined arguments. In 2001 Fried et al. proposed five major aspects for the identification of the frail under clinical conditions: – Unintentional weight loss – Low grip strength – Exhaustion – Slow walking speed – Reduced physical activity. Frailty is a reduction of physiological capacities not restricted to a defined organ system, but rather includes multiple physiologic systems and is not based on a unique pathogenetic process (Woodhouse and O’Mahony 1997). In this context, Rockwood et al. (1994) proposed a dynamic framework of frailty relying on the balance between health- and resourcemaintaining factors on the one hand and diseaseand disability-promoting factors on the other hand. A dysbalance within this framework forcing the system toward disability leads to an increased vulnerability of the patient for external stressors (Campbell and Buchner 1997). In this framework,
M. Wehling (ed.), Drug Therapy for the Elderly, DOI 10.1007/978-3-7091-0912-0_24, # Springer-Verlag Wien 2013
303
304
H. Burkhardt
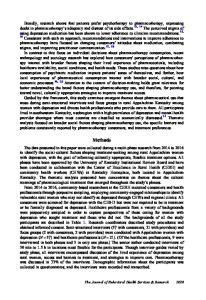
agingprocesses disease
neuroendocrine dysregulation malnutrition
sarcopenia reduced energy expenditure reduced metabolic rate
reduced maximal O2-uptake
reduced activity reduced gait-speed
reduced muscle strength
impairment
Fig. 1 The frailty cascade, including sarcopenia, reduced metabolic rate, malnutrition and reduced activity (Adapt
Data Loading...