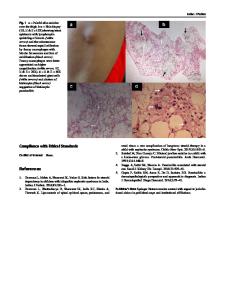
Spontaneous remission of genetic, apparent primary, FSGS presenting with nephrotic syndrome challenges traditional notio
- PDF / 2,274,241 Bytes
- 4 Pages / 595.276 x 790.866 pts Page_size
- 52 Downloads / 295 Views
LESSONS FOR THE CLINICAL NEPHROLOGIST
Spontaneous remission of genetic, apparent primary, FSGS presenting with nephrotic syndrome challenges traditional notions of primary FSGS Swe Z. M. W. H. Oo1 · Margaret E. Freese1 · Danniele G. Holanda2 · Christie P. Thomas1,3,4 Received: 27 May 2020 / Accepted: 11 August 2020 © This is a U.S. government work and its text is not subject to copyright protection in the United States; however, its text may be subject to foreign copyright protection 2020
Keywords FSGS · Genetic diagnosis · Foot process effacement · Spontaneous remission · TRPC6
The Case A 26-year-old Caucasian female was referred for new onset nephrotic syndrome (NS). She was well until early June 2018 when she developed bilateral leg swelling followed by swelling of her arms and face. About 2 weeks into her leg swelling she was seen by nephrology who noted peripheral edema, a serum creatinine of 1.1 mg/dl (CKD-EPI eGFR 69), a serum albumin of 2.7 gm/dl and a urine protein creatinine ratio (UPC) of 9 (Table 1). Her prior serum creatinine was 0.7 mg/dl in 2014. She was diagnosed with NS and started on furosemide. She underwent a kidney biopsy that showed focal and segmental glomerulosclerosis (FSGS) in 2 out of 47 glomeruli with focal mild interstitial fibrosis and tubular atrophy, and severe diffuse foot process effacement (FPE) on EM (see Fig. 1a–c). She was started on lisinopril and was referred to the Renal Genetics Clinic because of her reluctance to start prednisone.
Electronic supplementary material The online version of this article (https://doi.org/10.1007/s40620-020-00837-7) contains supplementary material, which is available to authorized users. * Christie P. Thomas christie‑[email protected] 1
Division of Nephrology, Departments of Internal Medicine, SE419 GH, University of Iowa Carver College of Medicine, 200 Hawkins Drive, Iowa City, IA 52242, USA
2
Departments of Pathology, University of Iowa Carver College of Medicine, Iowa City, IA, USA
3
Departments of Pediatrics, University of Iowa Carver College of Medicine, Iowa City, IA, USA
4
Veterans Affairs Medical Center, Iowa City, IA, USA
A 3-generation pedigree demonstrated that she has no family history of kidney disease (Fig. 2). Clinical examination showed that she has no extrarenal features, such as nail or patella abnormalities or hearing loss to suggest a syndromic form of FSGS. After meeting with a genetic counselor, she underwent genetic screening with KidneySeq™, a customized targeted renal gene panel [1]. Testing showed that she had a heterozygous missense variant in Transient Receptor Potential Cation Channel subfamily C Member 6 (TRPC6), a gene where pathogenic variants are a known cause of autosomal dominant FSGS [2] Fig. 1, panel D). The variant, p.Asn125Ser, the consequence of a c.374A > G transition is rare, is predicted to be deleterious, and in a previous study this variant demonstrated increased calcium transients in transfected HEK293 cells compared to the wild type gene (Supplementary reference 21). Further
Data Loading...